Cost

Drugs with high prices are often no better than...

Medicare for All lowers taxes for most Americans
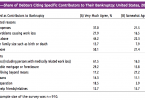
Overpriced health care too often means bankruptcy

Let’s have a prescription drug public option

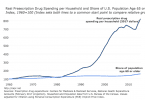
Out-of-pocket costs for Part D generics way up

Medicare encourages doctors to use costliest cancer...

National Academy of Sciences recommends drug price...

Drug coupons drive up overall health costs