

Enrollment

2026: Insurers predict that most people with Medicare...

Auto-enrollment in Medicare Advantage is a bad idea

Turning 65? When to enroll in Medicare

Administration expands Medicare special enrollment...

If you’re making a Medicare choice, don’t...

2020 Omnibus budget bill improves Medicare

Enrolling in Medicare? Here’s a checklist
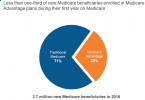
Most people choose traditional Medicare over Medicare...
