
MedPAC

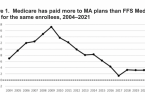
What if the government paid Medicare Advantage plans...
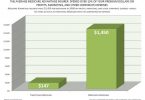
Senators ask Medicare agency why it is not holding...
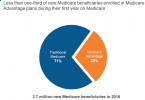
Most people choose traditional Medicare over Medicare...

UnitedHealth charged with enrollment fraud

Justice Department sues UnitedHealth Medicare...
