

Cost
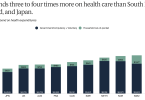
US continues to spend more for poorer quality care...

Poll: Many more older adults delayed care because of...

HCA hospital system is charged with overtreating...

How to ensure your hospital bill is correct

You can now buy hearing aids at the drugstore

Medicare Annual Open Enrollment: Beware of Bad Actors ...

2022: Health care costs threaten the well-being of...

Cancer patients face particularly severe medical debt
