

Medicaid

Who’ll lose health care after ACA repeal?

How to get dental care if you have Medicare

Trump HHS pick is fierce opponent of Medicare and ACA

Thankful for traditional Medicare? Call Paul Ryan

New and innovative home and community-based services...

How can we rely on paid caregivers?

8.3 million people benefit from both Medicare and...
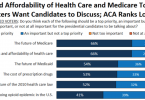
Access to affordable care top priority among voters
