Mortality

Genes play an important role in how long you live

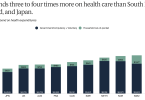
Why do Americans die younger than people in other...

With exercise, every move you make counts

2025: Could Americans be getting healthier?

Live longer, avoid ultraprocessed foods

Elevance Health sues to undo changes to Medicare...

Being mildly overweight in older age has its benefits

The choice between traditional Medicare and Medicare...