

Patent

Let’s make medicines a public good again

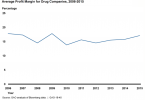
UCLA helps Pharma keep drug costs high
GAO: Drug prices continue to skyrocket

How Pharma keeps generics off the market

Allergan transfers patents to Native American tribe to...
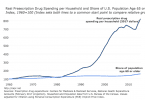
Drug costs eating into greater share of income
