

PhARMA

Hundreds of patient advocacy groups are Pharma shills

States focus on drug importation as way to rein in...

Pharma blocks state law requiring disclosure of drug...
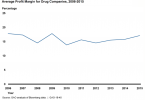
GAO: Drug prices continue to skyrocket
Trump’s pick to head HHS drove up insulin prices...

Reining in drug costs remains public’s top...

How Pharma keeps generics off the market

Senate bill would empower Medicare to reduce drug...
