

Reference pricing

Democratic Presidential candidates debate health care...
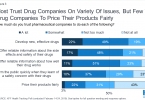
Majority of Americans do not trust pharmaceutical...

Sanders drug bill makes it easier for patients to...

What Trump will do about Part B drug prices

Congressman Doggett takes lead on Medicare drug price...

Amazon plans to sell and distribute prescription drugs

How the US should negotiate drug prices

Paying less for hospital care through reference pricing
