
In an op-ed for the New York Times, former Administrator of the Centers for Medicare and Medicaid...

In an op-ed for the New York Times, former Administrator of the Centers for Medicare and Medicaid...

David Dayen writes for The American Prospect on the horrific number of deaths at nursing homes...

Ricardo Alonso-Zaldivar reports for AP that fraudsters are trying to sell older adults and people...

Congress has just passed an $8 billion emergency spending package to help address the coronavirus...

With the coronavirus spreading quickly in the US and few federal efforts to date to contain it, the...

If you value your Medicare and Social Security benefits as much as the vast majority of Americans...
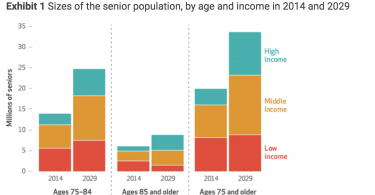
A new paper in Health Affairs projects that many middle-income older adults will not be able to...

Nearly 12 million people with Medicare also are enrolled in Medicaid. If you have Medicare and...

A recent paper by Community Catalyst’s Leena Sharma, Carol Regan and Katherine Villers...
What does it take to drive big health care system change? Trump’s HHS head, Alex Azar, recognizes...