
Caring for an older person with multiple needs can take a toll physically, emotionally and...

Caring for an older person with multiple needs can take a toll physically, emotionally and...

Howard Gleckman reports for Forbes on why everyone 65 and older should expect to need long-term...

The Program of All-inclusive Care for the Elderly (PACE) is a home and community-based program...

We are an aging population. And, caring for older adults is costly. Not surprisingly, family...

Since the start of the novel coronavirus pandemic, more than 46,000 people have died in nursing...

Katie Engelhart reports for California Sunday on what happened at Life Care Center of Kirkland, the...

The financial and emotional toll of caring for older adults has always been enormous. The novel...
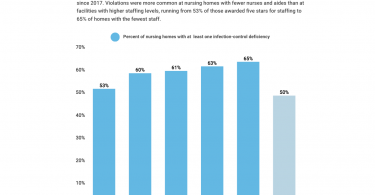
Jordan Rau reports for Kaiser Health News that for quite some time nursing homes have not been...

If you’re looking for free local resources to help older adults, your local Area Agency on Aging...

The US health insurance system has become increasingly privatized. One big trend is in the Medicaid...