
If your income is low, you might be able to get help paying your Medicare premiums and copays...

If your income is low, you might be able to get help paying your Medicare premiums and copays...

Many people do not appreciate how important Medicaid is for middle-class families, reports Ron...

Felice J. Freyer reports for Kaiser Health News on how some hospitals now provide at-home rehab...

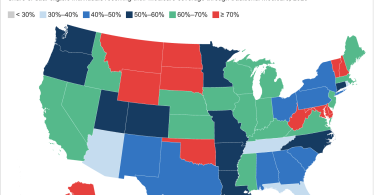
Medicare only covers about half of a typical person’s health care costs, leaving people with...

Maya Goldman reports for Axios on the risks of Medicare Advantage flex cards for people getting...

Medicare only covers about half of a typical person’s health care costs, leaving people with...

Caring for an older person with multiple needs can take a toll physically, emotionally and...

The next Covid-19 booster shot should now be available from your local pharmacy, health clinic or...
More than 12 million Americans with Medicare also have Medicaid. These “dual-eligibles”...

Millions of people max out their credit cards, and an increasing number max out because of a costly...