

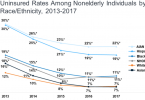
Uninsured

More than 4 in 10 Americans face cost barriers to care

2022: Health care costs threaten the well-being of...

Budget reconciliation: What’s happening with...

Coronavirus: Health insurers celebrate their most...

Coronavirus: Blame corporate health insurers for our...

Medicare for All would lead to a better performing...
Medicare for All addresses racial injustice

Up to 4 million will be uninsured if Medicare...
