Data

Why doesn’t HHS penalize pharmaceutical...

Coronavirus: Lack of timely data jeopardizes public...
2020: What you might not know about Medicare Advantage...

Half of health care spending goes to doctors and...
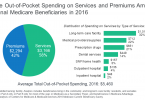
People with Medicare still spend an average of $5,500...

How do you choose a hospital?

PPIs found to increase risk of kidney failure

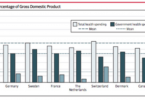
US health care system ranks last in meeting...